악성 종괴와 감별이 필요하였던 간의 혈관근지방종 1예
요약
간의 혈관근지방종은 대부분 무증상이며, 다양한 영상학적 소견으로 악성 질환과의 감별이 필요한 경우가 많다. 조영 초음파, 컴퓨터단층촬영 등으로 감별이 힘들다면 추가로 조직검사를 확인하는 것이 도움이 되며, 악성으로 변할 가능성이 높은 경우에는 수술적 치료가 필요할 수 있다.
중심 단어: 혈관근지방종; 간질환; 조영 초음파; 생검
Abstract
A 36-year-old female was referred for a huge heterogenous hepatic mass found on health check-up ultrasonography. She had no significant past medical history and was asymptomatic. All laboratory test including liver function test, tumor marker was normal. A contrast-enhanced ultrasonography, computed tomography, and magnetic resonance imaging revealed a hepatic mass 8 cm in size that occupied the right posterior segment. The lesion showed arterial enhancement, portal washout and well circumscribed margin. Based on these imaging findings, it was necessary to differentiate from malignant liver disease. Liver biopsy was performed. In the biopsy specimen, the tumor was composed mostly of epithelioid myoid cells and the fat cell component was inconspicuous, and positive for human melanoma black-45, which is common finding in hepatic angiomyolipomas. The patient underwent surgical resection and in observation in out-patient clinic.
Keywords: Angiomyolipoma; Liver disease; Contrast-enhanced ultrasonography; Biopsy
서 론
혈관근지방종은 간에서 발생하는 중간엽 종양의 일부로, 혈관, 평활근, 지방세포의 세 가지 성분이 다양하게 포함된 것이 특징이다. 원래 신장에서 가장 많이 발생하는 것으로 알려져 있으나, 1976년 Ishak의 첫 보고 이후로, 간 혈관근지방종의 보고가 이어지고 있으며, 국내에서는 약 16건이 보고된 바 있다[ 1, 2]. 환자별로 혈관근지방종의 혈관, 평활근, 지방세포의 비율이 다르기 때문에 영상 소견이 매우 다양하게 보고되고 있으며, 종양으로 오인되는 경우가 많다. 현재 혈관근지방종의 진단율은 약 25-52%에 불과하다[ 3]. 대부분 무증상이나, 일부에서는 크기 증가, 재발, 전이 등의 악성 변화가 보고되고 있어 수술적 치료가 필요할 때가 있다[ 4]. 저자들은 우연히 발견된 간종괴를 주소로 내원한 환자에서 조영 초음파, 전산화단층활영, 조직검사를 통해 간 혈관근지방종으로 진단한 환자를 경험하였기에 보고하고자 한다.
증 례
36세의 여자 환자가 건강검진으로 시행한 복부 초음파의 이상 소견을 주소로 내원하였다. 환자는 이전 병력이 없이 건강한 상태였으며, 호소하는 증상은 없었다. 신체 검진상 복부 압통 등의 특이 소견은 보이지 않았다. 혈액검사에서 B형간염, C형간염의 증거는 없었으며, 이 외 백혈구, 혈색소, 간기능 검사 수치는 모두 정상이었다. 종양 표지자는 모두 정상이었다(alpha-fetoprotein 1.9 ng/mL, carcinoembryonic antigen 0.51 ng/mL, carbohydrate antigen 19-9 4.9 U/mL).
이전 병원에서 시행한 복부 초음파검사에서, 우하엽 분절에 약 7 cm 크기의 경계가 뚜렷한 고에코성 종괴가 보였다( Fig. 1). 본원에서 간 초음파 및 조영 초음파를 시행하였고, 우하엽 분절에 8 × 7 cm 크기의 경계가 명확한 비균질한 종괴가 관찰되었다. 종괴는 우간정맥에 인접하였고, 동맥기에서 조영증강, 문맥기 및 지연기에서는 저에코성의 소견이 보였다( Fig. 2). 감별 진단을 위해서 간 컴퓨터단층촬영검사를 시행하였다. 우하엽에 8.7 × 7.3 cm 크기의 경계가 잘 구분되는 종괴가 보였으며, 조영 초음파 소견과 마찬가지로 동맥기에서 조영증강되고, 문맥기 및 지연기에서 저음영으로 관찰되었다( Fig. 3). 간세포암종을 감별하기 위하여 간자기공명영상검사를 시행하였고, T1 강조영상에서는 저음영, T2 강조영상에서는 고음영의 소견이었다. 컴퓨터단층촬영검사와 동일하게 동맥기에서 조영증강되고, 문맥기 및 지연기에서 저음영으로 관찰되었으며, 간담도기(hepatobiliary phase)에서 저음영이었다( Fig. 4). 악성을 감별하기 위하여 간생검을 실시하였다. 종양은 주로 상피근종세포(epithelioid myoid cell)로 이루어졌으며, 지방세포 성분은 많지 않았다. 상피모양세포(epithelioid cell)에서 호산구 양성 세포질(eosinophilic cytoplasm)과 다양한 크기의 핵이 관찰되었으며, 세포질에서 melan A와 human melanoma black-45 염색이 강양성 소견이었다( Fig. 5). 환자는 간 혈관근지방종으로 최종 진단되었고, 외과에서 절제술을 시행받았으며, 현재 외래에서 경과 관찰 중이다.
고 찰
일반적으로 혈관근지방종은 신장에 가장 많이 생기며, TSC1 (9q34), TSC2 (16p13) 같은 유전자 이상을 동반할 때가 많다[ 5]. 그러나 간에 생기는 혈관근지방종의 경우에는 유전자 이상이 동반되는 경우는 5-15%에 불과하며, 이 외 특별한 원인은 밝혀져 있지 않은 상태이다[ 4]. 본 증례에서 보는 바와 같이 대부분 무증상으로 우연히 발견되는 경우가 많으며, 혈액검사에서 이상 소견이 동반되는 경우도 극히 드물다. 현재까지 보고된 간의 혈관근지방종은 50세 미만의 여자에게 좀 더 많이 발생하는 경향이 있다[ 6]. 혈관근지방종은 이름에서 보는 바와 같이 혈관, 평활근, 지방세포의 세 가지 성분이 다양하게 섞여 있으며, 이들의 비율에 따라 영상 소견이 매우 다양하여 수술 전에 임상에서 정확하게 진단되는 경우는 약 25-52%에 불과하다. 결국 조직학적 생검이나 수술을 시행한 후에야 정확한 진단이 되는 경우가 많다. 특히 기저 간질환이 있는 경우나 간경변증이 있는 환자에서 혈관근지방종이 발생하면 간세포암 등으로 오인되는 경우가 많아 임상적으로 주의를 요한다[ 7]. 혈관근지방종은 복부 초음파 상에서 혼재성 에코 소견으로 보이는 경우가 많은데, 이는 지방세포는 고에코로 관찰되고, 반면 혈관과 평활근 부분은 저에코로 관찰되는데, 이들이 섞여있기 때문이다. 즉, 같은 혈관근지방종 환자라도 지방세포가 많을 경우 비교적 고에코로 관찰되고, 혈관이나 평활근 부분이 많은 환자라면 저에코로 관찰될 수 있다. 본 증례에서 시행한 것처럼 조영 초음파는 컴퓨터단층촬영 및 자기공명영상과 동일하게 유용하다고 보고된 바 있으며, 동맥기에는 조영증강되고, 문맥기 및 지연기에서는 조영감소가 된다[ 8, 9]. 특히 자기공명영상은 혈관근지방종을 진단하는 데 있어 가장 많은 정보를 제공해줄 수 있다[ 8]. 병리 소견으로는 평활근세포(myomatous cell)에서 염색되는 HMB-45 양성이 가장 특징적 소견이며, 이 외 혈관세포의 CD34 양성, CD63, CD67, desmin, S100, epithelial membrane antigen가 양성일 수 있으나 특이적이지는 않다[ 4]. 보통은 병리검사에서 혈관, 평활근, 지방세포의 세 가지 성분이 모두 관찰되면서, HMB-45가 양성일 경우 혈관근지방종으로 진단하게 된다[ 10]. 혈관근지방종은 기존에는 양성 종양으로 알려졌으나, 최근 일부에서 악성으로 진행한다는 보고가 있으며, 수술 부위의 재발, 타장기 침범, 전이까지 다양한 양상을 보인다[ 4]. 다년간 크기 변화가 없을 경우, 종양의 크기가 5 cm 미만일 경우, 기저 간질환이 없을 경우, 환자가 무증상일 경우에는 특별한 치료 없이 경과 관찰이 가능하다. 그러나 악성 종양과 감별이 어려운 경우, 크기가 커져서 증상을 유발하는 경우, 빠른 크기 변화를 보일 경우에는 수술적 제거가 필요하다. 특히 병리검사에서 높은 세포 분열의 특성을 보이면서 다형성 핵(pleomorphic nuclei)이 관찰되는 경우나, p53 돌연변이가 있을 경우 악성으로 진행할 가능성이 있으므로 추후에 추적 관찰검사가 필요하다.
Figure 1.
Ultrasonographic findings of hepatic angiomyolipoma. One mixed echoic nodule of 8 cm in size was seen in the right hepatic region. The lesion exhibited clear border, uneven echo, and reticular structure. 
Figure 2.
Contrast-enhanced ultrasonography of hepatic angiomyolipoma. The tumor showed inhomogenus hyperenhancing pattern in the arterial phase and iso- or hypoehoic during the portal and delayed phase. 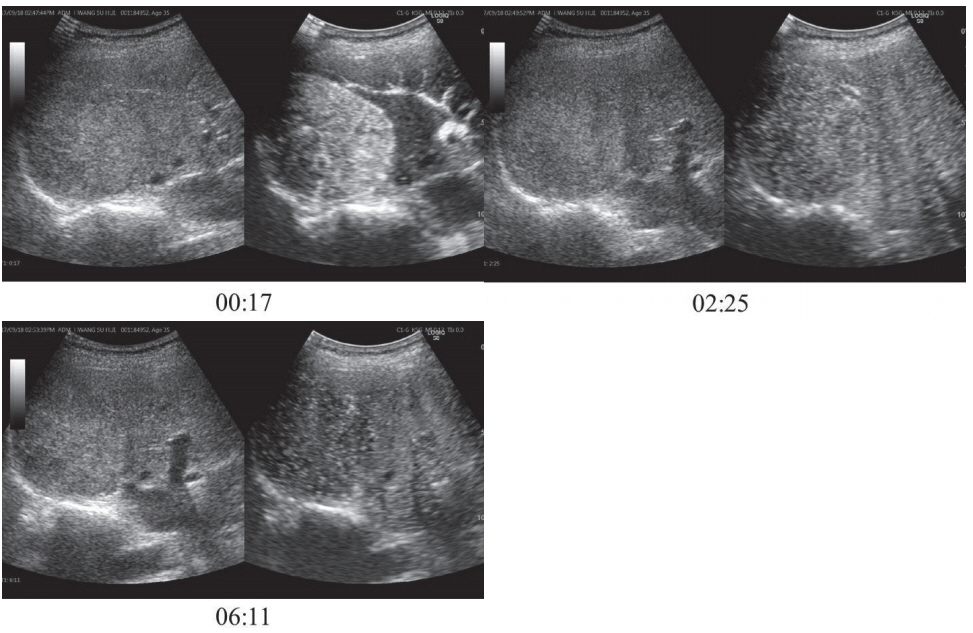
Figure 3.
Computed-tomography (CT) of hepatic angiomyolipoma. CT showed highly enhanced lesion in arterial phase, iso- or hypoechoic in portal phase. 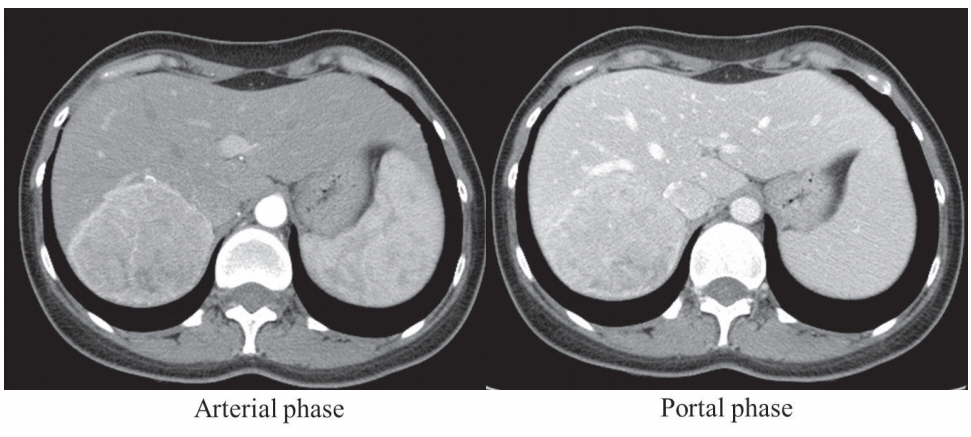
Figure 4.
Magnetic resonance image (MRI) of hepatic angiomyolipoma. (A) MRI showed 8 cm sized mass with T1 phase low, T2 phase high. (B) The lesion showed arterial enhancement, portal and delayed phase washout, and low signal intensity in hepatobiliary phase. 
Figure 5.
Pathologic findings of hepatic angiomyolipoma. (A) The tumor is composed mostly of epithelioid myoid cells and the fat cell component is inconspicuous, which is common finding in hepatic angiomyolipomas (HE stain, ×100). (B) The tumor shows epithelioid cells with abundant eosinophilic cytoplasm and variably sized nuclei. The epithelioid myoid cells are positive for Melan A and HMB-45 with strong granular cytoplasmic staining, supporting the diagnosis of angiomyolipoma (×400). 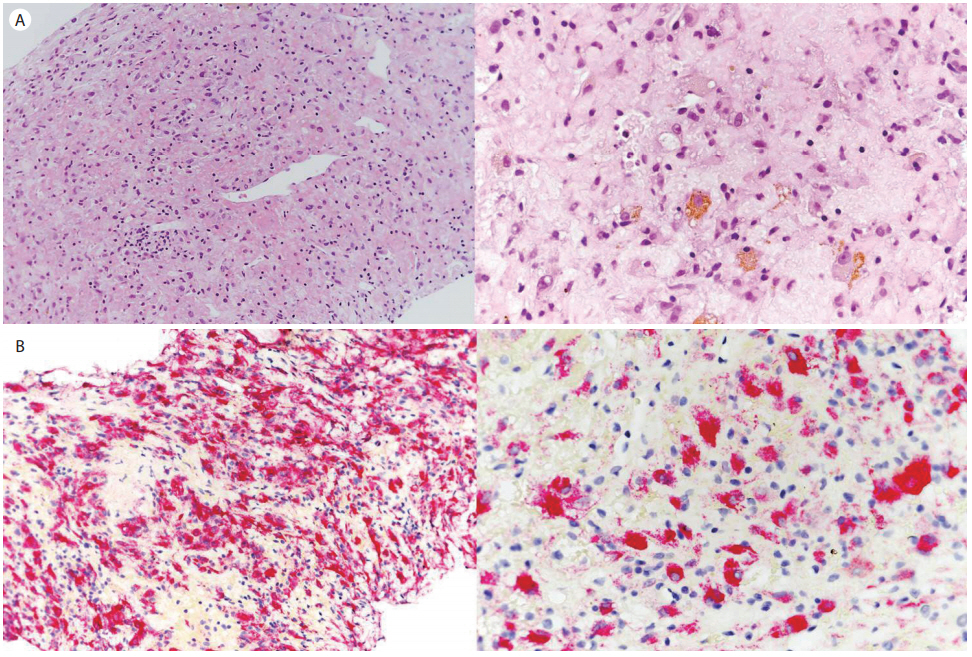
REFERENCES
1. Mani H, Van Thiel DH. Mesenchymal tumors of the liver. Clin Liver Dis 2001;5:219–257, viii.   3. Ding GH, Liu Y, Wu MC, Yang GS, Yang JM, Cong WM. Diagnosis and treatment of hepatic angiomyolipoma. J Surg Oncol 2011;103:807–812. 5. Tsui WM, Colombari R, Portmann BC, et al. Hepatic angiomyolipoma: a clinicopathologic study of 30 cases and delineation of unusual morphologic variants. Am J Surg Pathol 1999;23:34–48. 6. Du S, Li Y, Mao Y, et al. Diagnosis and treatment of hepatic angiomyolipoma. Hepatobiliary Surg Nutr 2012;1:19–24.  7. Zhong DR, Ji XL. Hepatic angiomyolipoma-misdiagnosis as hepatocellular carcinoma: A report of 14 cases. World J Gastroenterol 2000;6:608–612. 9. Li R, Zhang X, Hua X, et al. Real-time contrast-enhanced ultrasonography of resected and immunohistochemically proven hepatic angiomyolipomas. Abdom Imaging 2010;35:676–682. 10. Flemming P, Lehmann U, Becker T, Klempnauer J, Kreipe H. Common and epithelioid variants of hepatic angiomyolipoma exhibit clonal growth and share a distinctive immunophenotype. Hepatology 2000;32:213–217.
|
|