경동맥 초음파: 임상 의사를 위한 기본 영상 및 판독법
Abstract
Carotid duplex ultrasound or ultrasonography is an ultrasound-based noninvasive imaging technique to explore anatomic and hemodynamic details of the carotid arteries. B-mode scanning reveals carotid intima-media thickening and carotid plaque; pulsed-wave Doppler imaging, stenosis severity. Clinically, carotid intima-media thickness and plaque levels inform cardiovascular risk stratification and exact assessment of carotid stenosis severity often guides further therapeutic interventions. This review will present the imaging technique and interpretation of carotid duplex ultrasound as a real-world clinicians’ guide.
Keywords: Carotid arteries; Doppler duplex ultrasonography; Carotid intima-media thickness
중심 단어: 경동맥; 도플러 초음파; 경동맥 내중막 두께
서 론
경동맥 초음파는 비침습적으로 초음파를 이용하여 경동맥의 구조적 이상을 평가하는 검사 기법이다. 이는 임상적으로 두 가지 측면에서 적용될 수 있다. 하나는 경동맥의 포괄적인 접근으로서, 죽상동맥경화 정도를 평가하고자 할 때, 쉽게 초음파로 볼 수 있는 경동맥을 전체 동맥의 대표성을 가진 동맥으로 생각하여, 경동맥 내중막 두께(carotid intima-media thickness) 또는 플라크(plaque)로 개체의 죽상동맥경화 위험도 또는 전임상적 혈관병에 대한 예측을 하고자 하는 것이다[ 1- 4]. 다른 하나는 경동맥의 국소적인 접근으로서, 경동맥 협착의 위치와 정도를 평가하여 추가적인 치료가 필요한지 여부를 결정하고자 하는 것이다. 만약 경동맥 내중막 두께 검사만을 요구하였다면, 이는 내경동맥의 협착을 평가하는 도플러 초음파를 꼭 포함해야 하는 것은 아니다. 즉 협착을 평가하는 도플러검사를 함께 수행할 때는 경동맥 내중막 두께 검사가 아니라, 경동맥 초음파검사로 지칭함이 바람직한 용어의 사용이라 하겠다. 본 종설에서는 경동맥 초음파의 적응증, 기본 영상, 측정 및 판독을 검사를 수행하는 임상 의사의 관점에서 기술하고자 한다.
본 론
경동맥 초음파 적응증
경동맥 초음파는 다양한 임상 시나리오에서 시행될 수 있는데, 2006년 미국심초음파 학회와 미국혈관학회[ 5] 및 2016년 미국영상의학회[ 6] 적응증을 정리하면 표 1과 같다. 다만, 경동맥 내중막 두께 검사만 시행할 경우에는 중간 정도의 심혈관 위험도를 가진 환자에서 유용하며(예를 들면, 기존의 심혈관질환이 없는 위험도 6-20%인 사람, http://www.mdcalc.com/framingham-coronary-heart-disease-risk-score), 내중막 두께 측정 수치로 인하여 치료가 바뀔 가능성이 없다면 검사의 의미가 없겠고[ 7], 죽상동맥경화지 2011년 발표에서도 저위험 또는 고위험도 환자에서 혹은 위험도 평가를 위한 반복적인 검사(serial testing)에서는 적합하지 않은 것으로 평가하였다[ 8].
경동맥 초음파 기본 영상
피검자는 등과 머리를 바닥에 댄 편안한 자세에서 낮은 베개를 사용하여 목이 굽혀지지 않도록 하고, 검사하고자 하는 경동맥의 반대편으로 고개를 살짝 돌리도록 한다. 초음파 장비에서 선형 탐촉자(linear transducer, fundamental frequency ≥ 7 MHz)를 선택하고, 이미지 셋팅(carotid option, depth 4 cm, single focal zone, frame rate ≥ 25 Hz)을 맞춘다. 2008년 미국심초음파학회 권고에서와 같이 네 단계의 영상 순서를 따르는 것이 보편적이며( Table 2) [ 7], 공통적으로 B-mode를 이용하여 경동맥 플라크와 경동맥 내중막 두께를 평가하게 된다. 만약 첫 단계에서 경동맥 플라크가 발견되었다면, 4단계까지 굳이 가야 하나? 경동맥 내중막 두께의 수치와 관계없이 플라크가 있다는 것으로 이미 심혈관 위험도 평가에 양성으로 반영되므로, 위험도 평가의 목적에서는 내중막 두께를 더 측정하는 것이 헛수고 같다. 그러나 광의의 경동맥 초음파검사일 때는 다른 곳의 의미 있는 협착도 있을 수 있기 때문에, 병변이 많이 발생하는 내경동맥 분지 상부까지 경동맥 전반적인 이미징을 수행한다. 만약 B-mode상 의미 있는 협착(> 50%)이 의심되는 부위가 있다면, 도플러 속도 및 내경 협착 비율로 협착의 정도를 정량화하게 되는데, 2016년 미국영상의학회 권고에 따르면, 다음의 세 가지 영상기법을 순차적으로 적용하여(1. Bmode Grayscale; 2. Color Doppler; 3. Spectral Doppler), 총경동맥, 분지부, 내경동맥, 외경동맥, 척추동맥을 관찰하는 것으로 되어있다[ 6]. 이 중 척추동맥은 컬러 도플러상 색깔이 총경동맥과 같다면, 속도 측정을 생략하는 경향이 있다. 경동맥 내중막 두께란, 경동맥의 세 층(내막, 중막, 외막) 중에서 내막과 중막층의 두께를 의미한다. B-mode 초음파에서는 두 선 사이의 거리로 표현되는데(내강과 내막의 경계가 되는 선, 중막과 외막의 경계가 되는 선), 현재 임상에서 보급되어 사용되는 초음파의 해상도는 내막과 중막 사이 경계를 잘 구분하지 못하기 때문에 결국 내중막 두께를 묶어서 측정하게 된 것이다( Fig. 1). 경동맥 내중막 두께 측정을 위한 이미지는 “튜닝포크, 더블라인”을 만들기 위하여 노력하는데, 총경동맥 원위부 1 cm를 반드시 포함하는 far wall 더블라인이 잘 보이는 이완기말 정지 영상을 캡쳐하는 것을 권장한다. 경동맥 플라크란, 내중막 두께가 1.5 mm 이상 두껍거나, 부분적으로 내강으로 적어도 0.5 mm 또는 주변보다 50% 돌출되어 나온 것을 말한다[ 5]. 무언가 내강으로 돌출된 부분이 있다면, 한쪽 면에서만 보지 말고 장축, 횡축 이미지 등 다각도에서 접근해야한다. 상부로는 총경동맥에서 분지부로 이행하여 내경동맥과 외경동맥으로 나뉘어지는 내경동맥 중위부까지 관찰하는데, 내경동맥과 외경동맥은 위치, 크기, 도플러 파형으로 구분 가능하다( Fig. 2). B-mode로 협착이 의심되는 부위가 있을 때는 컬러 도플러로 혈류 가속을 평가하고, 또 협착 부위 전후로 pulsed-wave Doppler를 시행하며, 추가적으로 장축 및 횡축 스캔으로 경동맥 협착 부위를 가장 작고 동그랗게 만드는 B-mode 및 컬러 영상을 만든다.
경동맥 초음파 측정 및 판독
경동맥 내중막 두께의 측정 및 해석
경동맥 내중막 두께 측정의 부위와 횟수에 대하여는 논란이 있지만, 대체로 총경동맥 원위부 측정으로 대표성을 두고 있으며(distal 1 cm of common carotid artery far wall, not excluding plaque; R-wave gated), 다른 부위가 전반적으로 두꺼워진 것은 따로 기술할 수 있다[ 7]. 총경동맥 원위부를 택한 것은 어떤 특정 부위가 다른 부위보다 낫다는 뚜렷한 증거가 없는 상황에서 총경동맥 원위부가 다른 부위보다 이미지를 만들기 쉽고, 재현성이 뛰어나다는 장점이 있기 때문이다. Far wall을 택한 것은 near wall에서 발생 가능한 허상(excess gain, blossoming)을 피할 수 있기 때문이다. 심전도상 R wave 직전 이완기말은 내경이 가장 작은 반면 내중막 두께는 가장 두꺼운 시기이다. 경동맥 내중막 두께는 상기한 부위를 확대, 두 선 간의 거리를 수직으로 측정하여 그 측정 횟수로 나누어 평균값을 구하거나, 탑재된 소프트웨어를 이용하여 반자동적으로 구한다. 한국인의 정상 경동맥 내중막 두께에 대한 보고가 있는데[ 9], 정확히는 성별/연령별 정상치에서 75th percentiles 이상이면 위험도를 올린다고 평가하며 ( Table 3), 대개는 내중막 두께 ≥ 0.9 mm에서 위험도를 산정한다.
경동맥 플라크의 측정 및 판독
플라크는 횡축 및 장축 이미지를 만들어 존재 유무를 먼저 파악하며, 만약 존재하면 위치, 크기, 에코 성상(acoustic shadowing 포함)을 가능한 기술한다. 이차원적 단면에서 삼차원적 플라크 분포를 기술하는 데는 분명 한계가 있으며 그림으로 나타내기도 한다. 심혈관 위험도 평가에 있어서 내중막 두께 측정보다 플라크 존재 여부가 더 중요하다는 보고도 있다[ 10]. 가능한 플라크에 대한 정보를 자세히 기록하는 이유는, 에코 음영이 있는 경우 심혈관질환 발생이 상대적으로 높았고[ 3], 저에코 플라크의 경우에 허혈성 뇌졸중 발생이 더 높았다는 보고도 있으며[ 11], 결국 총 플라크 양이 허혈성 뇌졸중과 연관이 있기 때문이다[ 12].
경동맥 협착 정도의 측정 및 판독
경동맥 협착 정도를 평가하기 위해 두 가지 접근법을 병행하는 것이 도움이 된다. 하나는 도플러를 통한 혈류 속도 측정, 다른 하나는 B-mode를 통한 좁아진 내강 비율 측정이다. 좁은 혈관을 지나는 혈류의 속도는 빨라지게 되는데, 속도가 빨라질수록 혈관 조영술 상의 협착 정도가 심해진다는 것은 잘 알려져 있고, 그 임계가 되는 수치는 50% 이상 협착일 때 최대 속도 125 cm/sec, 70% 이상 협착일 때 최대 속도 230 cm/sec이다[ 13] ( Table 4). 죽상동맥경화로 좁아진 내강 비율을 구함에 있어서 미국식(North American Symptomatic Carotid Endarterectomy Trial, NASCET)과 유럽식(European Carotid Surgery Trial, ECST)은 상이하다[ 14]. NASCET가 병변이 없는 정상 부위를 기준으로 협착을 평가하였다면, ECST는 병변 부위의 횡축에서 바로 협착 정도를 평가한다. 유럽식은 양성 리모델링된 전체 내강이 분모가 되므로 협착이 상대적으로 더 심하게 계산될 수 있는 단점에도 불구하고, 정상 경동맥을 찾아 따로 이미징하여 대조하는 번거로움을 피할 수 있기 때문에 임상적으로는 더 널리 적용되고 있다( Fig. 3). 경동맥 초음파에서 50% 미만의 협착이 진단된 경우에는 대개 위험 인자를 조절하면서 관찰하지만, 증상이 있는 환자에서 경동맥 초음파상 70% 이상의 협착이 진단된 경우에는 이차적인 치료(예를 들면, 경동맥 내막절제술, 경동맥 스텐트시술)를 고려하여 의뢰하는 것도 필요하다[ 15].
결 론
가속화되는 고령화 사회에 동반되는 각종 만성 질환은 죽상동맥경화성 혈관 질환의 위험인자이므로, 죽상동맥경화증은 가장 흔히 진료실에서 만나는 질환 군이 되었다. 경동맥 초음파는 전임상 단계의 죽상동맥경화, 임상적 심뇌혈관질환에 대한 위험도 예측 및 국소적인 병변을 파악하는데 비침습적이고 반복 가능한 일차적인 접근법으로 점차 널리 보급되고 있다. 이에 본 종설은 기본 단계로 임상의가 쉽게 수행하고 해석할 수 있는 경동맥 초음파 영상, 측정 및 판독법을 소개 하였으며, 추후에 보다 우리 실정에 맞는 표준화된 검사법 및 보고서를 정립하는데 있어 기초가 될 것으로 사료된다.
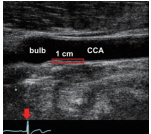
Figure 1.
Longitudinal plane with tuning fork view and double-line sign. Distal 1 cm of the far wall of the common carotid artery: inner line is between the lumen and intima; outer line is between the media and adventitia. The carotid-intima media thickness is the distance between the two lines. 
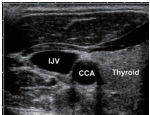
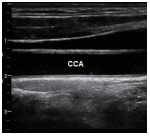
Figure 2.
How to differentiate the internal from the external carotid artery. PS, peak systolic; ED, end-diastolic. 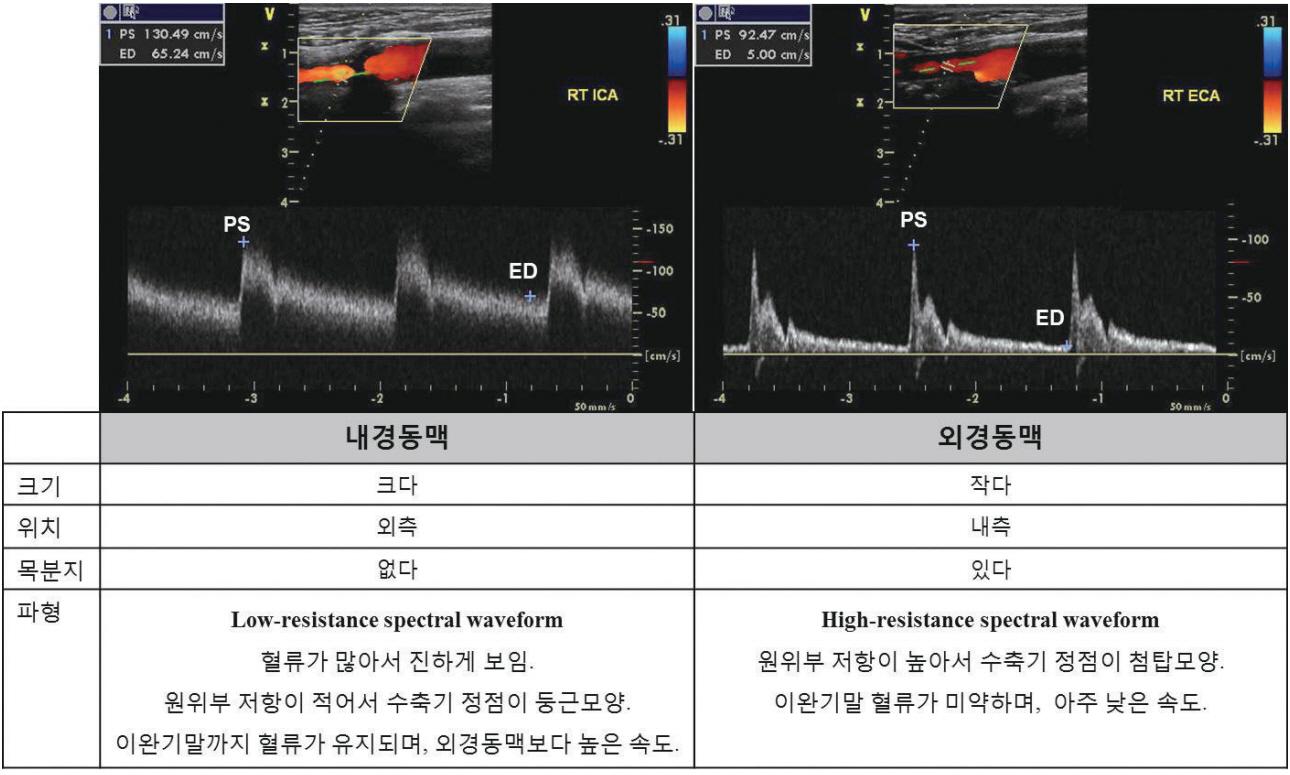
Figure 3.
Difference between NASCET and ECST in measurement of internal carotid artery stenosis. NASCET, north american symptomatic carotid endarterectomy trial; ECST, european carotid surgery trial; CCA, common carotid artery; ICA, internal carotid artery. 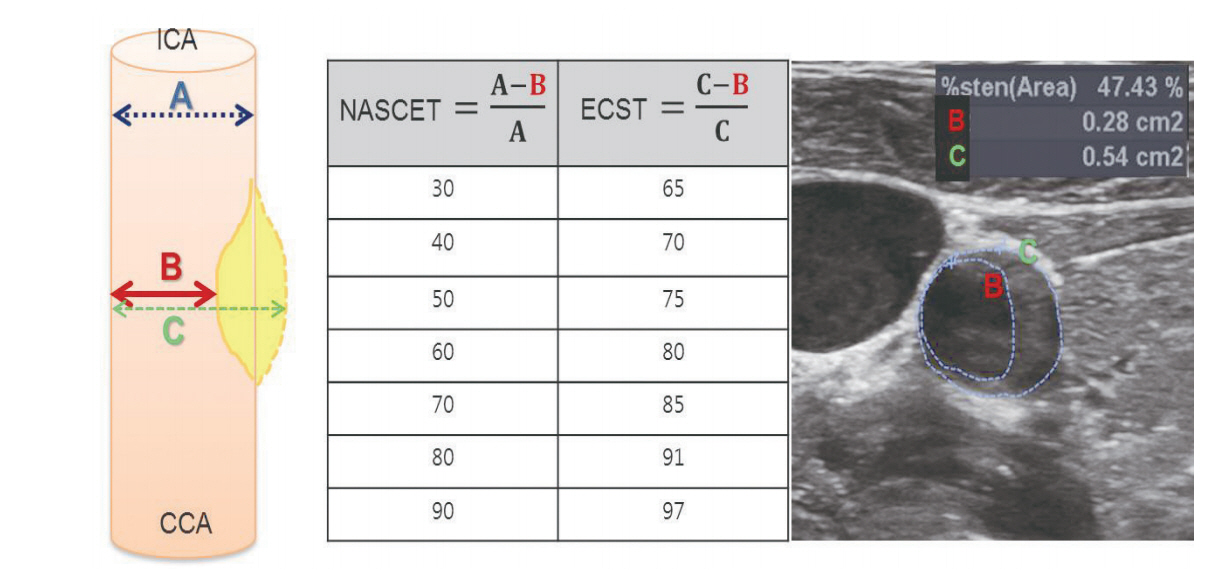
Table 1.
Indications for carotid ultrasonography
|
1. Hemispheric neurologic symptoms: stroke, transient ischemic attack, amaurosis fugax |
|
2. Non-hemispheric or unexplained neurologic symptoms |
|
3. Syncope, seizures, dzziness |
|
4. Suspected subclavian steal syndrome |
|
5. Cervical bruits |
|
6. Pulsatile neck masses |
|
7. Neck trauma |
|
8. Suspected carotid artery dissection, arteriovenous fistula, or pseudoaneurysm |
|
9. Vasculitis involving extracranial arteries |
|
10. Screenings: atherosclerosis elsewhere, history of head and neck radiation, known fibromuscular dysplasia, Takayasu arteritis |
|
11. Carotid reconstruction after extracorporeal membrane oxygenation bypass |
|
12. Preoperative evaluation for major cardiovascular surgery |
|
13. Postoperative evaluation for cerebrovascular revascularization: carotid endarterectomy, stenting, or carotid-to-subclavian artery bypass graft |
|
14. Follow-up evaluation for proven carotid disease |
Table 3.
References of carotid intima-media thickness in Korean populations (2011 Korea Research Institute of Standards and Science)
|
Sex |
Age |
Percentiles values of mean carotid intima-media thickness (mm)
|
|
25th |
50th |
75th |
90th |
100th |
|
Male |
40s |
0.54 |
0.60 |
0.68
|
0.77 |
1.11 |
|
50s |
0.60 |
0.68 |
0.79
|
0.90 |
1.69 |
|
60s |
0.63 |
0.70 |
0.82
|
0.94 |
1.90 |
|
70s |
0.64 |
0.75 |
0.85
|
0.98 |
1.43 |
|
Total |
0.60 |
0.69 |
0.80
|
0.92 |
1.90 |
|
Female |
40s |
0.51 |
0.56 |
0.64
|
0.72 |
0.89 |
|
50s |
0.60 |
0.67 |
0.76
|
0.86 |
1.39 |
|
60s |
0.64 |
0.73 |
0.81
|
0.92 |
1.80 |
|
70s |
0.64 |
0.75 |
0.85
|
1.02 |
1.60 |
|
Total |
0.60 |
0.69 |
0.79
|
0.90 |
1.80 |
Table 4.
Diagnosis of internal carotid artery stenosis severity using Doppler ultrasound [ 13]
|
Degree of stenosis |
ICA
|
ICA/CCA, peak systolic velocity ratio |
|
Peak systolic velocity (cm/sec) |
End-diastolic velocity (cm/sec) |
|
Normal |
< 125 |
< 40 |
< 2.0 |
|
< 50% |
< 125 |
< 40 |
< 2.0 |
|
50–69% |
125–230 |
40–100 |
2.0–4.0 |
|
≥ 70% |
> 230 |
> 100 |
> 4.0 |
|
100% |
Undetectable |
NA |
NA |
REFERENCES
3. Hunt KJ, Evans GW, Folsom AR, et al. Acoustic shadowing on B-mode ultrasound of the carotid artery predicts ischemic stroke: the Atherosclerosis Risk in Communities (ARIC) study. Stroke 2001;32:1120–1126.   4. Den Ruijter HM, Peters SA, Anderson TJ, et al. Common carotid intima-media thickness measurements in cardiovascular risk prediction: a meta-analysis. JAMA 2012;308:796–803. 5. Gerhard-Herman M, Gardin JM, Jaff M, Mohler E, Roman M, Naqvi TZ. Guidelines for noninvasive vascular laboratory testing: a report from the American Society of Echocardiography and the Society for Vascular Medicine and Biology. Vasc Med 2006;11:183–200. 6. AIUM Practice Parameter for the Performance of an Ultrasound Examination of the Extracranial Cerebrovascular System. J Ultrasound Med 2016;35:1–11.
7. Stein JH, Korcarz CE, Hurst RT, et al. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr 2008;21:93–111. 8. Society of Atherosclerosis Imaging and Prevention Developed in collaboration with the International Atherosclerosis Society. Appropriate use criteria for carotid intima media thickness testing. Atherosclerosis 2011;214:43–46. 9. Bae JH, Seung KB, Jung HO, et al. Analysis of Korean carotid intima-media thickness in Korean healthy subjects and patients with risk factors: Korea multi-center epidemiological study. Korean Circ J 2005;35:513–524. 11. Mathiesen EB, Bønaa KH, Joakimsen O. Echolucent plaques are associated with high risk of ischemic cerebrovascular events in carotid stenosis: the tromsø study. Circulation 2001;103:2171–2175. 12. Mathiesen EB, Johnsen SH, Wilsgaard T, Bønaa KH, Løchen ML, Njølstad I. Carotid plaque area and intima-media thickness in prediction of first-ever ischemic stroke: a 10-year follow-up of 6584 men and women: the Tromsø Study. Stroke 2011;42:972–978. 13. Grant EG, Benson CB, Moneta GL, et al. Carotid artery stenosis: gray-scale and Doppler US diagnosis--Society of Radiologists in Ultrasound Consensus Conference. Radiology 2003;229:340–346. 14. Staikov IN, Arnold M, Mattle HP, et al. Comparison of the ECST, CC, and NASCET grading methods and ultrasound for assessing carotid stenosis. European Carotid Surgery Trial. North American Symptomatic Carotid Endarterectomy Trial. J Neurol 2000;247:681–686. 15. Brott TG, Halperin JL, Abbara S, et al. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease. Stroke 2011;42:e464–e540.
|
|